Shrewsbury maternity scandal: Repeated failures led to deaths
 PA Media
PA MediaCatastrophic failures at an NHS trust may have led to the deaths of more than 200 babies, nine mothers and left other infants with life-changing injuries.
Senior midwife Donna Ockenden examined maternity practices at Shrewsbury and Telford NHS Trust (SaTH) over 20 years.
Her report found that babies' deaths were often not investigated and grieving parents were not listened to.
This meant, she said, "failures in care were repeated" and some mothers were even blamed for their own deaths.
SaTH has apologised to affected families and described the report as "deeply distressing". It said many changes highlighted by Ms Ockenden had already been introduced.
Kayleigh Griffiths, whose daughter Pippa died in 2016, said words from the trust "aren't going to be enough".
"Once we stop getting stories [which we've had] right up until today of poor care in SaTH, we're not going to be settled that any improvements have been made," she said.

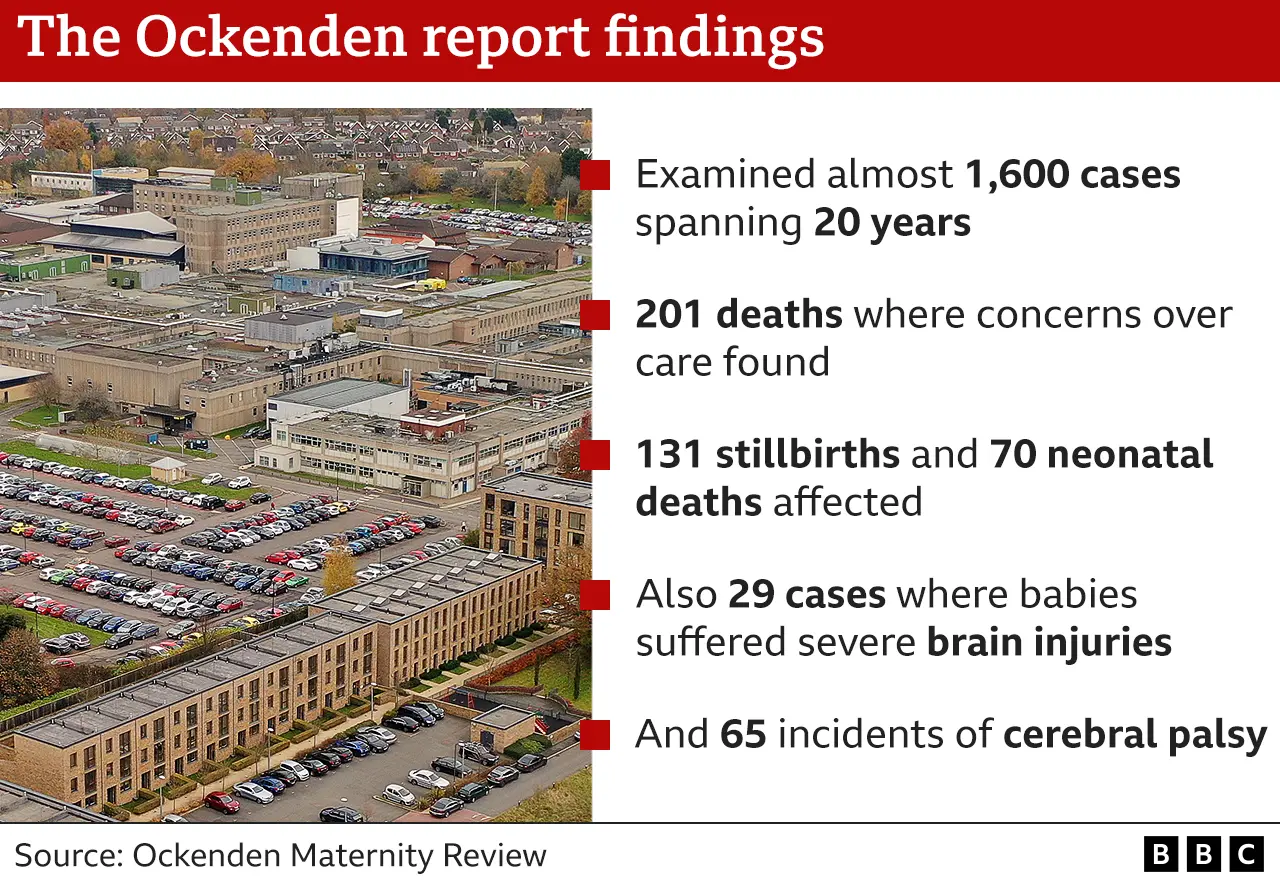
The review, which examined almost 1,600 cases, is thought to be largest of its kind in NHS history.
Severe brain injuries
It revealed 201 babies could have survived had SaTH provided better care, related to 70 neonatal deaths and 131 cases where babies were stillborn.
There were also 29 cases where babies suffered severe brain injuries and 65 incidents of cerebral palsy.
Rhiannon Davies, whose daughter Kate died in 2009, said the numbers themselves did "not not tell the whole story" of the impact on families.
Ms Ockenden said: "We now know that this is a trust that failed to investigate, failed to learn and failed to improve.
"This resulted in tragedies and life-changing incidents for so many of our families."
Post-it notes
Speaking in the House of Commons on Wednesday, Health Secretary Sajid Javid told MPs in one case the hospital trust had kept important clinical information on post-it notes, which were then swept into the bin by cleaners.
 PA Media
PA MediaIn all the cases identified by the inquiry, as well as nine mothers' deaths, it found better care "might" or "would reasonably be expected" to have made a difference.
Ms Ockenden cited examples of ineffective monitoring of foetal growth and a culture of reluctance to perform Caesarean sections as repeated problems which "resulted in many babies dying during birth or shortly after".
"The reasons for these failures are clear," she said. "There were not enough staff, there was a lack of ongoing training, there was a lack of effective investigation and governance at the trust and a culture of not listening to the families involved."

Key findings:
- A culture where mistakes were not investigated and a failure of external scrutiny
- Parents were not listened to when they raised concerns about the care they received
- Where cases were examined, responses were described as lacking "transparency and honesty"
- The trust failed to learn from its mistakes, leading to repeated and almost identical failures
- A culture of bullying, anxiety and fear of speaking out among staff at the trust "that persisted to the current time"
- Caesarean sections were discouraged, often leading to poor outcomes
In all, Ms Ockenden identified 60 specific improvements that could be made at SaTH and said there could be "no excuses" going forward.
The review found a culture of not investigating mistakes, with hundreds of instances where SaTH failed to appropriately examine deaths or undertake serious incident investigations with mistakes being "inappropriately downgraded".
Between 2011 and 2019, 40% of stillbirths and 43% of neonatal deaths did not even have an investigation. Of those cases that were examined, the Ockenden team graded the reviews as poor in almost half of stillbirths and over a third of neonatal cases.
In 2020, West Mercia Police also launched an investigation, called Operation Lincoln, to explore whether there was evidence to support a criminal case against the trust or any individuals involved.
Det Ch Supt Damian Barratt said the investigation was "very much active", although no charges had yet been brought.
Analysis
By Michael Buchanan, Social Affairs correspondent
The numbers are enormous, shocking even for those of us who long suspected there was something far wrong with the care at the trust. But the crucial thing to remember is that what the failings highlight are individual families who've grieved in private and at times been lied to by a trust that seemed uninterested in helping them to understand what happened or to learn any lessons.
Reading the report, there seems at times to have been an almost casual disregard for life - mothers have explicitly told me of being told, you'll be fine, you're young, you can have another child.
The central question now is how does the trust convince the women of Shropshire that it's currently providing a safe service - Donna Ockenden's remarks about care and culture in the trust in 2022 raise significant questions about the ability of the leadership team there to drive through the many changes that are clearly needed.
Blame mothers
On those occasions where cases were investigated, the trust failed to identify areas for improvement and missed opportunities to learn.
Ms Ockenden added the trust had a tendency to blame mothers for poor outcomes, and even in some cases for their own babies' deaths.
The inquiry was first commissioned in 2017 following a campaign by two families who had lost their babies.
Richard Stanton and Rhiannon Davies's daughter Kate died hours after her birth in March 2009, while Kayleigh and Colin Griffiths' daughter Pippa died in 2016 from a Group B Streptococcus infection.
As the bereaved gathered to hear the findings, Ms Griffiths said the report was "200-odd pages of harmed families".
"That's a disgrace that they haven't learned when we've told them what the issues were.
"We visited Pippa this morning before we came, and we said 'this is what we've done for her'."
The Nursing and Midwifery Council (NMC) said the report's findings were "appalling".
 PA Media
PA Media"Each of these cases is a family tragedy, with some affected more than once," Chief Executive Andrea Sutcliffe said.
"It's down to the sheer determination and bravery of grieving families that these systemic failures have now been recognised. Women and families should have been listened to and taken seriously far sooner."
Former health secretary Jeremy Hunt, who commissioned the review after being approached by the families, said the findings were "far worse" than he could have imagined and he hoped it would be a "wake-up call".
Responding to the findings, current Health Secretary Sajid Javid said they painted a "tragic and harrowing picture of repeated failures in care".
'Tragedy and distress'
Addressing the House of Commons, he said Ms Ockenden had described to him "basic oversights at every level".
"Rather than moments of joy and happiness for these families, their experience of maternity care was one of tragedy and distress," he said.
Mr Javid also highlighted "serious issues" with the culture at SaTH.
He told MPs that two-thirds of staff surveyed reported witnessing cases of bullying, while some staff "withdrew their co-operation with the report within weeks of [its] publication".
 UK Parliament
UK ParliamentMs Ockenden had earlier said staff were frightened to speak out about failings amid "a culture of undermining and bullying", with staff advised by trust managers not to take part in a "staff voices" initiative set up to assist the investigation into what went wrong.
Responding to the Health Secretary's statement in the Commons, Shadow Secretary for Patient Care Feryal Clark said: "No woman should ever have to face going into hospital to give birth and not know whether she and her baby will come out alive.
"These were not just one off or isolated incidents of negligence, this was institutional failure of a system which failed to take up the many opportunities to realise they had a serious problem."
Conservative Telford MP Lucy Allan asked if what had been seen at SaTH was indicative of a culture where "women's voices were not heard" and asked Mr Javid to do "everything he can" to increase accountability of senior management across the NHS.
Mr Javid said: "I want to reassure her we will implement all the recommendations in this report but even broader than that, when it comes to women's voices that will be at the heart of the upcoming women's health strategy."
Liberal Democrat MP for North Shropshire, Helen Morgan said the deaths of these babies "must not be in vain", while Philip Dunne, Conservative MP for Ludlow, praised the tenacity of his former constituents Richard Stanton and Rhiannon Davies following the death of their baby Kate.
Prime Minister Boris Johnson earlier said his heart went out to the families, adding: "Every woman giving birth has the right to a safe birth."
Donna Ockenden's review calls for increased funding, training and accountability across maternity services as well as improved post-natal care and care for bereaved families.
"The legacy of this review should be a maternity service across England that is appropriately funded, well-staffed, trained, motivated and compassionate and willing to learn from failings in care," she said.
"There should never again be a review of this scale, in both numbers and the length of years across which these concerns remained hidden."
Louise Barnett, chief executive at the Shrewsbury and Telford Hospital NHS Trust said, the report was "deeply distressing".
"We offer our wholehearted apologies for the pain and distress caused by our failings as a trust," she said.
"We have delivered all of the actions we were asked to lead on following the first Ockenden report, and we owe it to those families we failed and those we care for today and in the future to continue to make improvements, so we are delivering the best possible care for the communities that we serve."

During his speech to the Commons, Mr Javid also highlighted how "multiple opportunities" to address issues were ignored by regulators, with the Care Quality Commission only rating maternity services as inadequate for safety in 2018, which he said was "unacceptable".
Ms Ockenden similarly outlined how local commissioners failed to identify problems at the trust, while national regulators and external bodies failed to grasp the extent of what was going on.
The NHS Shropshire, Telford and Wrekin Clinical Commissioning Group (CCG) said it deeply regretted the "horrific experiences these families went through and that we failed to provide the care they deserved".
"We will work with our partners across the health and care system to ensure that further improvements are made in light of this report, and will continue to take all actions necessary to ensure women who use our maternity services receive the best care."
If you are affected by issues raised in this article, help is available through the BBC's Action Line.
Follow BBC West Midlands on Facebook, Twitter and Instagram. Send your story ideas to: [email protected]